Initial concepts and ideas
Yesterday was the second set of student presentation at The Glasgow School of Art. The purpose of this session was for the students to present their initial concepts in relation to their themes (social isolation, anticipatory care, re-enablement and partnership and communication). They were looking for feedback from practitioners, older people and and carers about how close these concepts are to creating the life older people would like, the suitability of the concepts in responding to the theme, and their practicality in the south side of Glasgow.
We had a full house of students, a few practitioners in the morning session and more in the afternoon. This meant feedback was limited in the morning and become more fruitful in the afternoon – reiterating that this project really is a collaboration/co-design project – without feedback and practitioners ideas and perspectives it is hard to evolve the concepts into relevant and practical ideas.
Work in the interm
Since the last presentations some of the students have been to visit the Nan McKay Hall where older people get together (see previous blog post), a GP at Midlock Medical Center, practitioners and older people at Cornerstone, and kept in touch with practitioners by email or phone.

Presentations
Each group presented and asked for feedback. We will make the presentations available on the blog asap so you can see the visual presentation of the concepts and how they would fit into a scenario that an older person may experience.


Social Isolation
The first group up was the social isolation group, they presented 3 ‘low technology’ ideas about engagement in the community when you are socially isolated, but are finding this a hard topic to address because it can be quite vast. Following this presentation this group are going to focus on narrowing the scope of the theme and develop concepts that respond directly to the older people’s profiles they have developed.
Furthermore, IRISS are providing some evidence support to assist the group in conceptualizing this issue – focusing on what the literature says about what is useful in overcoming social isolation and loneliness, what meaningful interactions might be as well as the use of technology.
View the presentation: 31_10_ Social Isolation
Anticipatory care
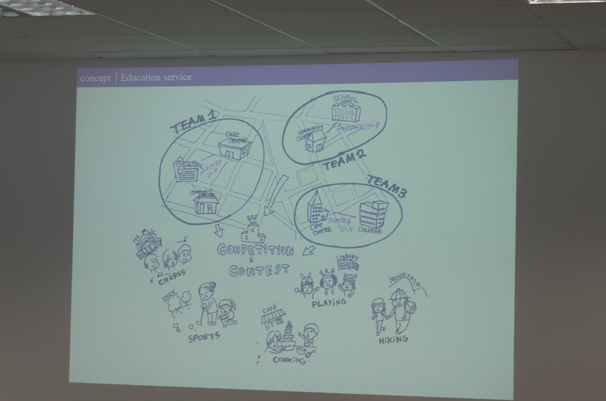
The anticipatory care group have decided to focus upon one area of anticipation – this being thinking, talking and being in contact with ‘old age’ in early years. This group believe that as a culture we don’t think about or anticipate our old age until it is imminent – this is not helped by poor representation of older people in the media and negative portrayals of older people as vulnerable, frail and isolated.
To address this, the group is interested in developing an awareness raising campaign, which would include activities that bring older people and younger people together through primary and secondary school settings. The aim of this being to break down barriers around knowledge and appreciation of old age, as well as possible inhibitions and fear between these two age groups. This approach really pushes the perspective of anticipatory care back to when people are growing up and what young people want their life to be like when they are older. So although not addressing anticipatory care needs right now, this team are looking more at a futures and generational perspective so the problem experienced at the moment could be alleviated in the future.
Reablement
This group presented 7 concepts called:
- Swapping and sharing
- Reablement buddy
- House swapping
- Guerrilla gardening
- Audio recording
- Generation mixer
- Skills sharing
One of the things this group has found difficult is getting to grips with what reablement means in a health setting as we were unable to pursue access to older people who are working with the NHS to enable themselves due to time an ethical constraints.
Therefore this groups has focused on ideas with people who still need support but are possibly not at the acute end of this issue. As a result, most of their ideas are community based – a factor they are going to take into consideration when developing these ideas further (concepts are currently too close to the social isolation group).
View the presentation: layout pres. lunedi.2
Partnership working and communication
This group presented 3 concepts:
- Link – referred to placing someone who has both health and social care knowledge in a GP’s surgery to act as a first point of contact and support a person to navigate the service landscape.
- Core team database – looked at combining the social work and health databases but making them person centered so that each person was able to have access and contribute to their records. It also considered employing a team of staff to make sure no one fell through the possible cracks between the two databases.
- The Hub – was the less developed of the three ideas but the one idea that most practitioners became quite excited about! The practitioners shared lots of ideas with the students as to what could be in the Hub, how it could work, and what would be there. The concept refers to a local area (hub) that people already use to go about their daily tasks – such as collecting their pension or buying food. The idea involves incorporating representatives from health and social work (or people with this kind of knowledge) than can signpost people to services that can support them or take them as these services would be in the Hub. What was stressed in this concept is that is is more of a community approach to people’s needs with health and social care a secondary (albeit important) element.
View the presentation: Concept_Ideas Partnership working and communication group
Summary
All of the groups have taken a community perspective when developing these concepts rather than a health or social service based response. This chimes with the underlying approach which focuses on the inclusion of the experiences and aspirations of older people and carers – it is these factors that the students are able to design for or towards, rather than the services expectations.
More work needs to be done by the students and practitioners to understand how the concepts could possibly complement existing networks, behaviours, actions or services and reconstitute them in some way. They also need to be made contextually relevant to the south side of Glasgow.
In the interim (2)
Ian Grout (the course leader) summarised and visualised how each of the theme’s concepts could sit together into a whole proposal for the future of care. The students need to consider this proposal and decide if they see their themes taking this kind of overall shape. As well as refining the concepts that gained positive feedback, they will work on the overall story of their ideas at the next group session on Wednesday.
Next presentation
The next presentation session will be held in one of the cares centers the south side.
We are keen to ensure that people who use services and their carers are engaged in the project as much as possible – especially now that ideas are beginning to form. As such we hope that the change of venue will encourage as many people to attend as possible to provide feedback that will help shape and refine the concepts – and so that we can ensure that the concepts are of most relevance to the people that count the most – older people and their carers.
Thanks for the summary Gayle – it’s really appreciated.
Hi Everyone
I was very interested in your presentation on Monday. You had a lot of information and I would like to look more closely when it is on the blog.
I have since been thinking about your perspective of anticipatory care, and in particular the interpretation of care.
I think that your idea of educating and integrating at a young age is very good. But is this care? In my ‘health-care’ world care comes at a later stage than this – at the time when a need has been identified. For us ‘anticipatory care’ for older people starts with identifying vulnerable and those ‘at risk’ of health difficulties.
Interested to hear your views!
Clare
Hello Clare, thank you for commenting !
I just posted our presentation.
Re Partnership working and communication
1) Think in general a problem would be staffing it, in the current financial climate and council tax freezes it is unlikely that a large number of new posts would be created unless it could be proved to be more efficient. Maybe would need pilot studies and staff reallocated from other duties?
There are over 1000 GP practices in Scotland http://www.isdscotlandarchive.scot.nhs.uk/isd/5384.html. Link staff would likely have to serve more than one practice in dense city populations or cover a wide geographical area if based in a rural setting (The Scottish Highlands and Islands are particularly challenging). Think a segment of Social Workers would already consider themselves as the ‘link’ on acting as an advocate for the service user and liasing with various professions/services on their client’s behalf. There are already Social Service staff who specialise in e.g. Mental Health issues or assisting eldery people return to home or care after hospital stays so these kind of staff are already working very closely with the health system – maybe their experience would be helpful in forumlating new proposals for building on what works or what needs improving?
2) Core team database. You’re rather assuming that ‘health’ and ‘social work’ have just one database each. Local Authorities in Scotland use different recordings systems. Health has a myriad of different systems e.g. Primary Care Mental Health may keep records just for the context of their involvement – GP’s cannot usually access this data electronically, information is only given by one to other professionals when the permission is granted by the service user or where they are at risk. There are very strong confidentiallity rules regarding patient data, so these would need to be considered in addition to any technical challenges involved in accessing the merged data.
Comments are closed.