For an overview of the approach we took in this project check out the Approach applied in KiP page. This page explains that the process we were working through was to ‘learn’, ‘plan’ and ‘do’ together. This meeting was our first opportunity to learn about each other and share what we knew about heart failure. Our goals for the day were:
- Connecting up and building relationships
- Sharing expectations about what we want to achieve
- Agreeing how we want to work together
- Agreeing homework and next steps
We achieved these goals by working through this programme.
Connecting up
For our ice-breaker we asked people, in pairs, to ask each other:
- Why did you come along today?
- What is one thing you are really quite good at?
- What is a random or interesting fact about you?
After hearing what their partner had to say we asked people to talk to someone else.
Sharing expectations
Traditional approaches tend to start with identifying a proposed end point and working back to devise a plan of activities. However, this approach does not tend to allow time for project outcomes to be considered by everyone in the group. Designing a project in terms of the outcomes people hope to achieve, can challenge traditional ideas of project management. I particularly like the view that,
“An approximate response to a well considered problem is worth a great deal more than an exact answer to an approximate problem.” (Alison Petch, IRISS Director, Ardoch House, Jan 2014).
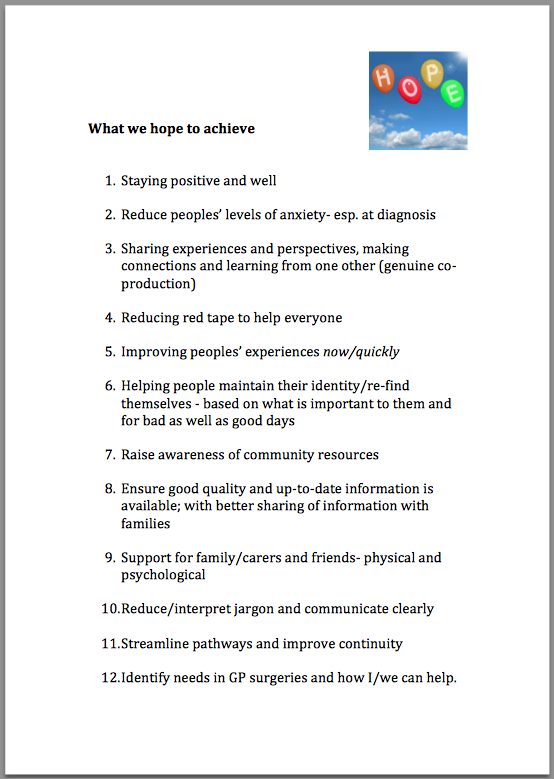
With this group, sharing expectations proved to be a useful exercise. It grounded us in reality and reminded us all why we were there. This helped bring the group together. This is a synthesised version of what we decided we wanted to achieve together.
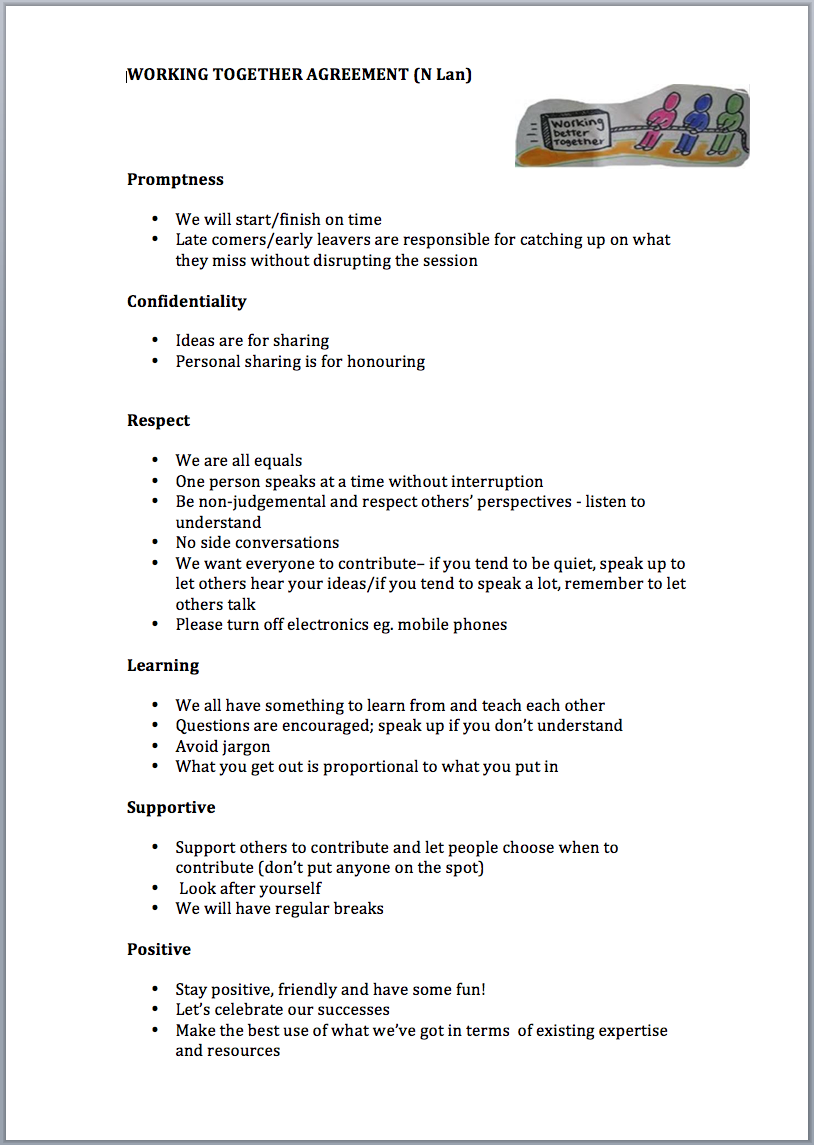
Working together agreement
In line with the principles of co-production, we asked the group to create a working together agreement. We gave them a suggested version and asked them to discuss whether there was anything in it they wanted to keep, amend or add. This is what was agreed:
Communication
We discussed what would help group members communicate effectively with each other during and between meetings (some of which fed into the final version of the working together agreement). Different aspects included:
- Remember to listen as well as speak
- Show respect for everybody
- Like idea of a project blog – but access denied/not available for some. Would be good to receive an email if a new blog post. Some in the group were also keen to contribute to the blog themselves which was encouraged.
- Good laugh and fun!
- Stairs!!!
- Use of jargon – problematic
- Noted that Chest Heart and Stroke have already produced a Glossary – a ‘Jargon buster’ type publication.
We also proposed a ‘parking lot’ idea, as a space to identify words or terms that the group considered get in the way of effective communication. At the first meeting ‘co-production’ was identified as one of those words! In addition, holding up ‘red cards’ if group members wanted others to stop when they didn’t understand was suggested, however the group decided this approach wasn’t necessary.
Introducing co-production
We played a short film, ‘The parable of blobs and squares‘ to introduce the concept of co-production. An alternative film you might want to use is ‘Co-production’ by SPICE.
https://www.youtube.com/watch?v=egav5xjb-lg
After watching this film we discussed in small groups what we do in our everyday lives that is co-produced, and the benefits of this kind of activity. We didn’t ask people about the challenges but they brought this up. Here’s a summary of their thoughts:
The benefits:
- It pools skills and experiences
- Nobody can do everything
- There is someone who can help – who can do what you can’t do
The challenges:
- You can become too reliant on others’ strengths, for example, doing things for children or for partner (and then they may no longer be there)
- It’s important to share your strengths with others
Exploring person-centred care and support
During the day we also explored what ‘person-centred care and support’ meant to people. As part of this, we asked everyone to reflect on what person-centred care meant to them. Prompts to help people, included three questions:
- What’s been good person-centred care?
- What could have been better?
- What help or support have you received that has mattered the most to you?
We asked people to write answers to these questions on a card and place it in an envelope. These were then passed around the group until the music stopped, people then read aloud what was written inside.

Completed cards on person-centred care
Summary of responses:
- What’s been good person-centred care?
- practical support from friends and having someone to talk to
- nurse took time to sit with me and explain things
- not being slotted in to a process
- different professionals involved in my care working together and being kept informed
- What could have been better?
- being given more information about side effects of medication
- to have been asked
- information sharing amongst professionals
- more information for the family
- What help or support have you received that has mattered the most to you?
- GP knowing me and taking time
- partner, friends and family
- my thoughts and views being acknowledged
- getting a diagnosis and treatment that is helping
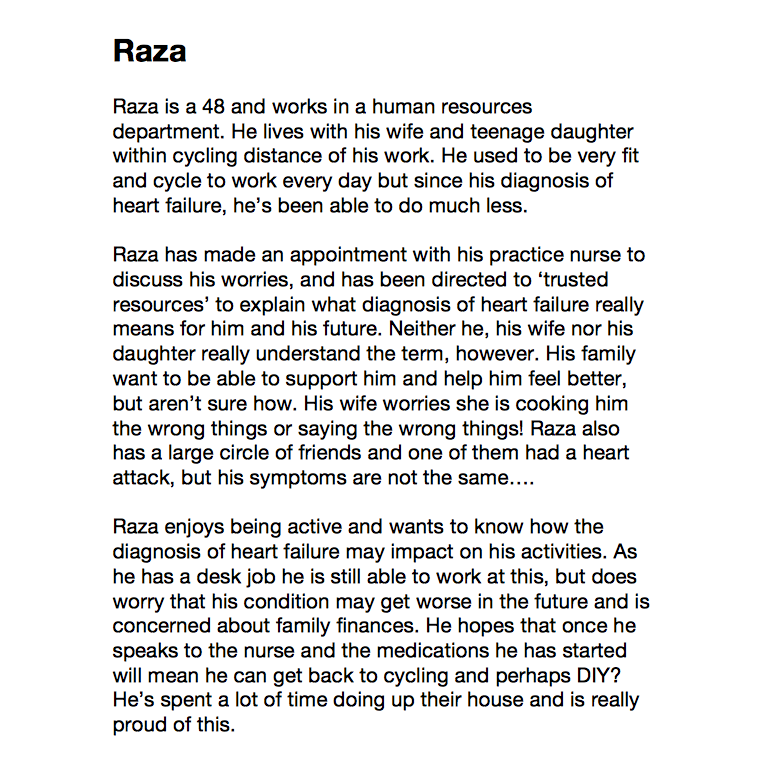
Next, we worked in small groups to identify initial ideas that people thought could improve support for people with heart failure. We were mindful that most of the group were meeting for the first time, so exercises were devised so that group members could draw upon their own experiences, but did not need to share them. For this reason, we created ‘personas’ or characters, devised with the help of Chest Heart and Stroke, to map pathways (or experiences) from pre- to post- diagnosis. Here are the personas we used.
Persona 1: Raza
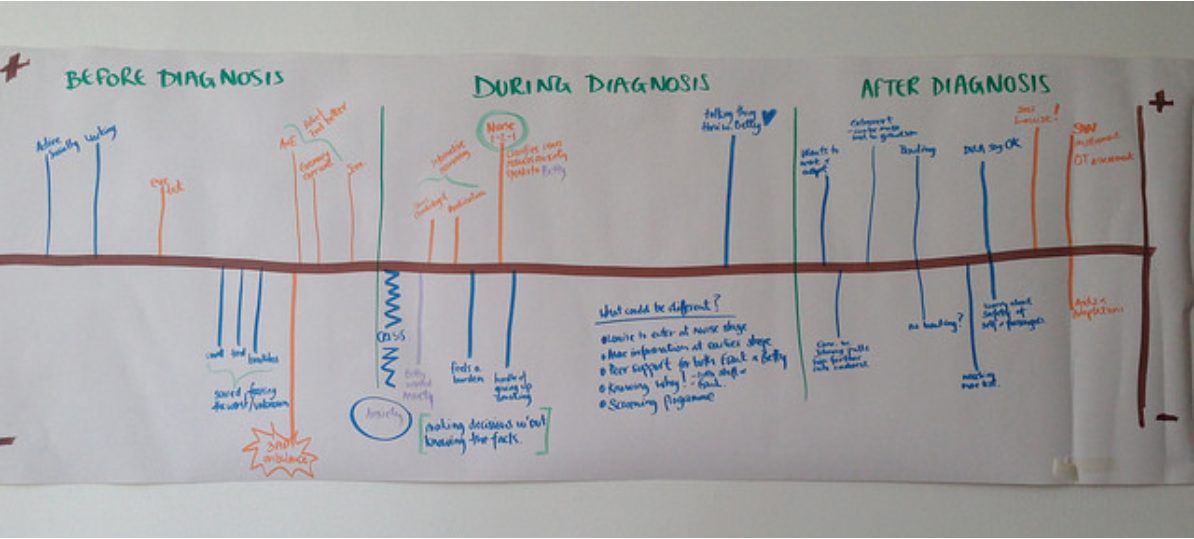
Persona 2: Frank
Persona 3: Molly To create these pathways we used lining paper and asked groups to plot key points for each of their personas to identify positive and negative experiences at: pre-diagnosis, diagnosis and post-diagnosis stages of heart failure. They were then asked to reflect on the experience they had plotted and discuss how the experience could have been improved. This discussion was also recorded on the maps. These are the experience maps drawn for each persona.
To create these pathways we used lining paper and asked groups to plot key points for each of their personas to identify positive and negative experiences at: pre-diagnosis, diagnosis and post-diagnosis stages of heart failure. They were then asked to reflect on the experience they had plotted and discuss how the experience could have been improved. This discussion was also recorded on the maps. These are the experience maps drawn for each persona.
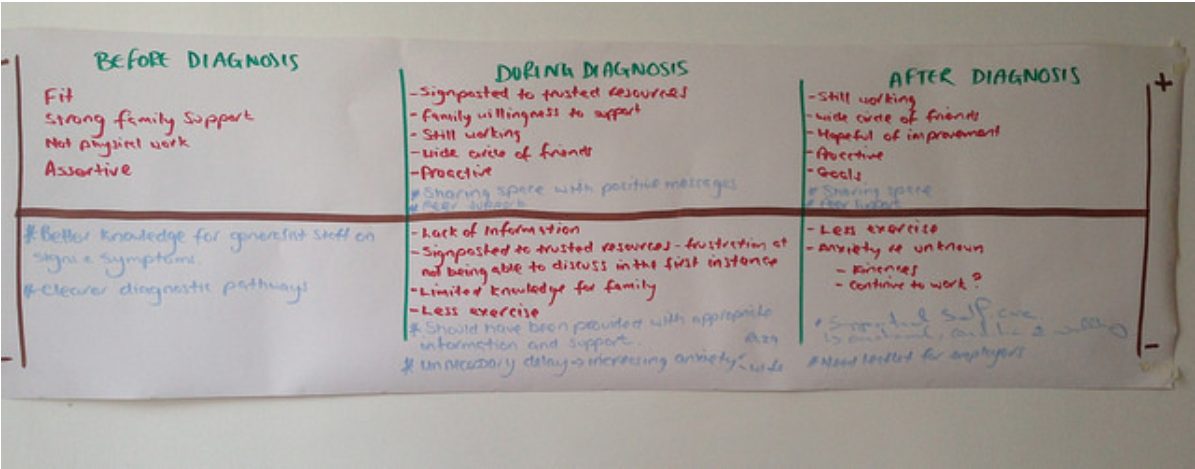
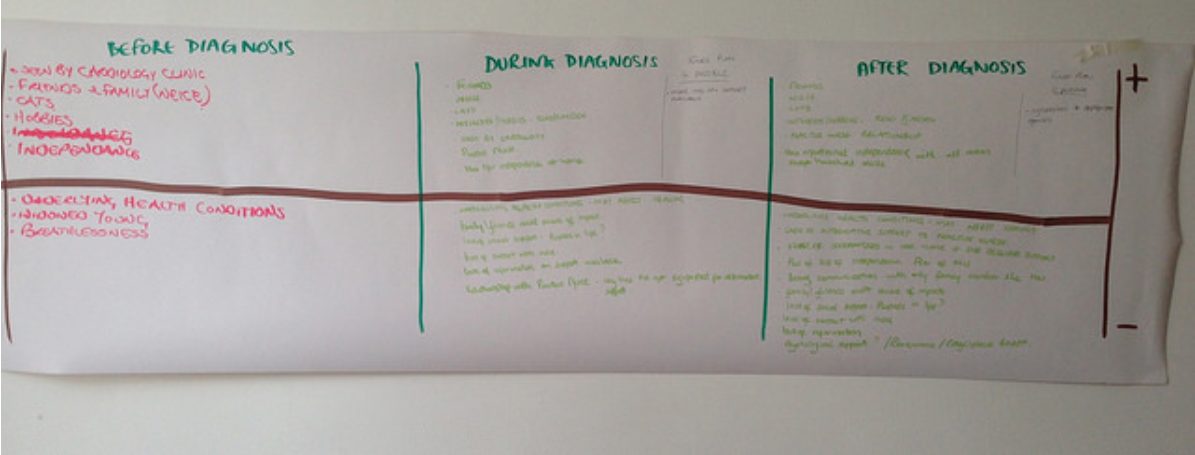
Ideas for improvement included:
Before diagnosis
- better knowledge of signs and symptoms for generalist staff
- clearer diagnostic pathways
- screening programme
During diagnosis
- more information at an earlier stage
- peer support – reassurance and positive messages
- heart failure nurse involved earlier
After diagnosis
- managing underlying health conditions
- social support
- information and reassurance
- support for self-care
- information for employers
Future meetings: getting the group to help set the agenda
Inspired by one of IRISS’ D-cards we decided to ask the group to help set the future agenda. We adapted the D-Card about ‘letting go of control‘ for this purpose. This adaptation involved asking small groups to think about several questions. Here are the questions and some of the responses:
- What else do we need to know/learn about to bring back to the group?
- how to connect agencies eg cardiology community
- how to raise awareness with public and with GPs
- Who can help us understand and learn this information?
- GPs
- public health information person
- Chest Heart and Stroke
- Others with the condition
- Is this knowledge within the group?
- knowledge of what works and what doesn’t
- What other expertise do we need to invite to join the group?
- mapping what’s out there
- examples of good things others have done
- What do we need to do between now and the next session to make some/all of this happen?
- talking to others with the condition
- recruit a GP
- develop a clear statement of why we are here and what we are going to do
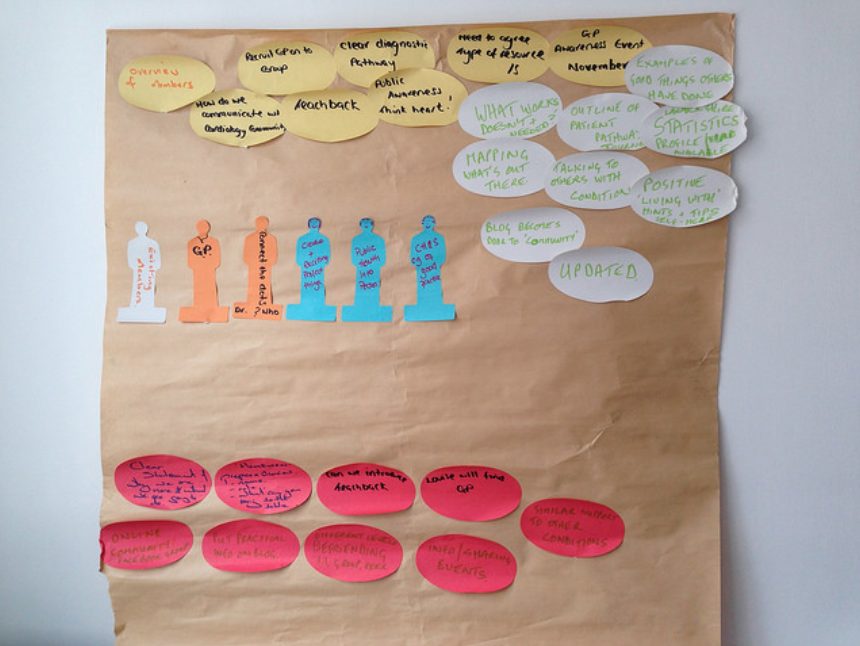
Group feedback on ‘setting the agenda’
From this discussion the group identified these 16 improvement ideas that could inform group activities.
Homework for next time
A good place to start we felt was asking group members to begin with themselves. We asked them to keep a journal/diary of personal reflections on the following and bring back 3 key insights to share next time:
- What person-centred care means to me in my life (or care and support that is centred around me)
- What person-centred care and support should look like
However, the group suggested an addition. This was to produce a personal profile for next time highlighting why they were here and what they could bring to the table.
Profiles of group members
Evaluation and feedback
We went for an ‘evaluation-lite’ approach, asking small groups to reflect on their gut reaction to the day and to feedback to the whole group using: smiley, not so sure, and unhappy faces.

We also asked people to share their thoughts about what went well during the session, what could have been better and what people will take away from the day. This is what people said:
What went well?
- Sharing experiences
- Like the room
- Group has gelled and everyone has contributed
- Going off at tangents was helpful
What could have been better?
- Tea!
- A bit longer for activities (though others were happy with this)
What will you take away from today?
- Less of a feeling of being on my own.