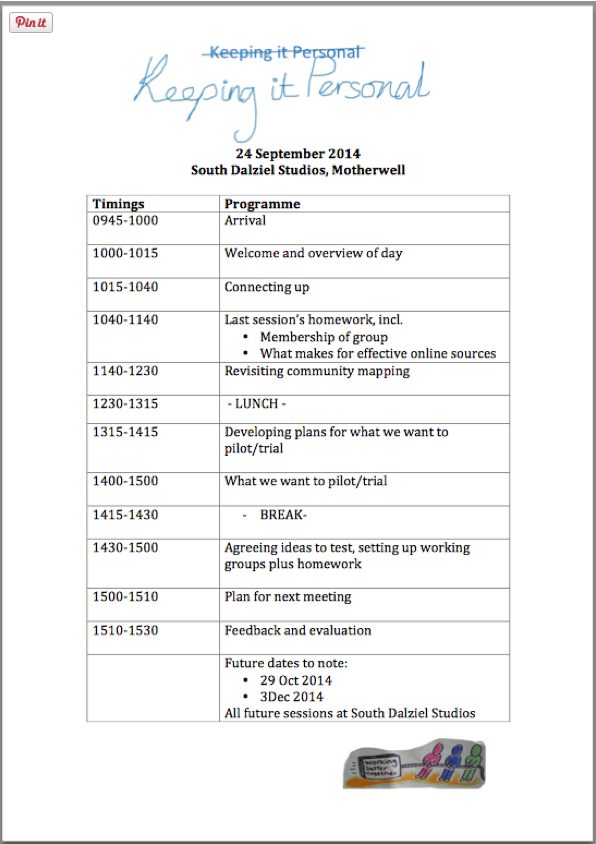
So now it was time to identify the ideas we wanted to develop and create plans to make these ideas a reality. We did this by working through this programme and having these goals:
{kind=link}
- Revisit community mapping and effective communication
- Develop and agree improvement ideas to trial
- Agree homework and next steps
Connecting up
Music is a great connector. To get everybody talking, relaxed and to get to know each other just that bit little more we asked group members to talk in pairs about their favourite songs and repeated this three times. People had great fun revealing why, for example, Eric Clapton’s ‘You Look wonderful Tonight’ was so special to them, or what it was about Queen that they loved (as well as their experiences of seeing them live!). We used spotify or YouTube for the whole group to listen together.
Last session’s homework – feedback from group
This session lasted beyond the time allocated in our programme. However, I decided to let it run as I thought it useful to let the group hammer out some of these issues. It seemed to help them really decide what were the most crucial things they wanted to focus on during the rest of the day. However, we then had to adapt and re-jig the remainder of the programme.
The homework (as based around the idea that online resources for people with heart failure are not particularly good) led to a group perception that good information gets mixed in with the bad, and accurate with mis-information. The group also identified that:
- It’s often hard to find through online searches/not known about
- People not signposted to relevant info
- It’s too negative/scary
- It’s too full of jargon
- It can be very confusing eg. American-based or out of date or, as already mentioned, downright wrong
When searching for different search terms people found:
- If you search for ‘Heart’ alone in North Lanarkshire Council website this brings up schools etc. It’s not until about the 5th line that you get anything relevant
- North Lanarkshire Council search for ‘heart disease’ brings up events eg on fundraising, and not links to heart failure
- ‘Heart’ is used as a prefix for many things (e.g. Hearts football club)
- Information is only as good as what goes in (if information is poor, a loss of credibility results)
Resources people identified as ‘good’ were:
- Chest Heart and Stroke resources – with one describing their newsletter as a ‘saviour’ with practical information
- British Heart Foundation resources
- Cardiomyopathy Association resources
- ‘Patient part’ of European Society of Cardiology
- Heart Failure Matters website, informed (?) by support groups with heart failure (with links to British Heart Foundation)
- Agreed that links from trusted websites (such as Chest Heart and Stroke and British Heart Foundation) to others provides quality assurance
- Ones without jargon and clear layout
Resources people identified as ‘not so good’ were:
- Resources that aren’t welcoming
- Ones that are too clinical (even the ‘good ones’ can be too clinical sometimes)
- NHS resources cited as the most negative – ‘very scary’ or boring
- We want to learn more from others’ experiences
- People can have different personal experiences- but there are also strong similarities in issues faced eg poor experiences with GPs and late diagnosis (a recurring theme); heart failure patients are often angry at diagnosis; services don’t talk to each other in the NHS/they are fragmented.
- Good to have different resources for different people at different times eg Facebook, doctors, meetings with others
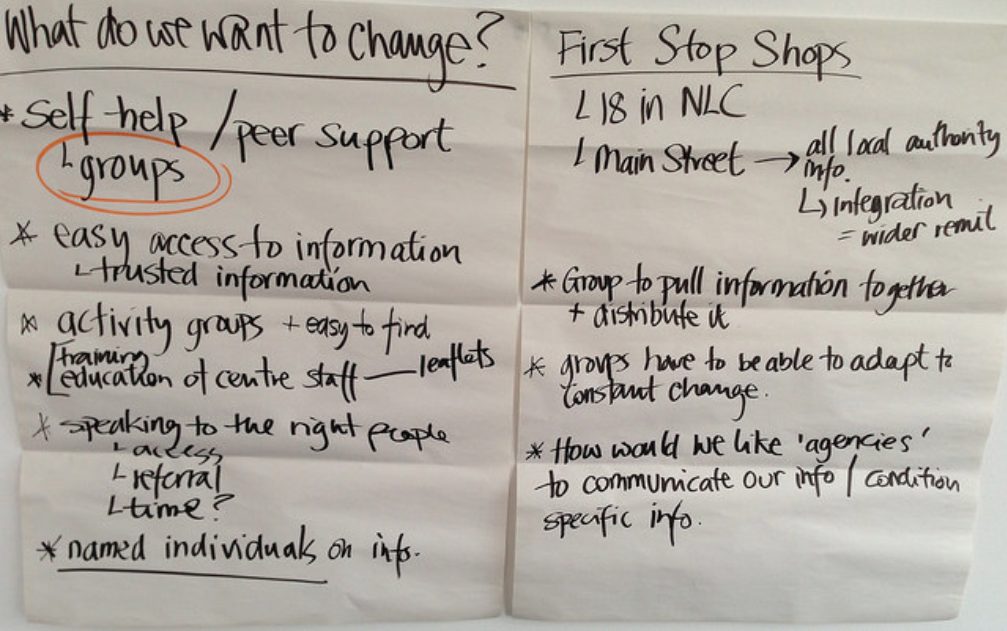
- We’d like:
- Joined up pathways
- A one-stop shop?
From this discussion we identified that people considered heart failure not as a disease, but a response to something else. They believed that earlier diagnosis and increased availability of appropriate support could improve the experience for those affected. This became the key issue for this group.
Consequently, the group felt that GPs should be the lynch pin for person-centred care. However, some of the group wondered whether GPs always fully explored patients’ medical history. They feared that without this understanding there was a risk of misdiagnosis and inappropriate treatment. Group members felt they had experienced reading wrong information. For example, having fluid on your legs may lead you to a self-diagnosis of heart failure, but it could also be the result of another condition. There was also the possibility of misdiagnosis due to different approaches to testing.
This discussion identified that fear can be a barrier to people visiting their GP when they have symptoms. The group was clear that accurate information, a checklist even, was needed. However, the approach would need to provide a positive message that if you do have heart failure there are things that you can do. And according to group members, that shouldn’t automatically mean being advised to give up your job – which can lead to depression.
For those with lived experience in the group, it was often only when they met a heart failure nurse that things began to fall into place. However, it was recognised that the heart failure nurses can only do so much and can be overstretched. Plus, their focus is not on prevention. By this point, things have advanced and opportunities may have been missed to prevent deterioration. Group members’ experiences of attending a cardiologist every year for 25 years, had left them feeling that there was little they could do for themselves that would make a difference. In hindsight, they believed this was not the case and that they had missed opportunities to keep themselves well. One group member’s son, who had the same inherited condition, had the benefit of her hindsight and was keeping fit and taking the right medicines.
We also discussed that health literacy can be a big problem. People felt there was a lack of consistency around receiving written information and that patients often didn’t know the right questions to ask.
Is it all about better education?
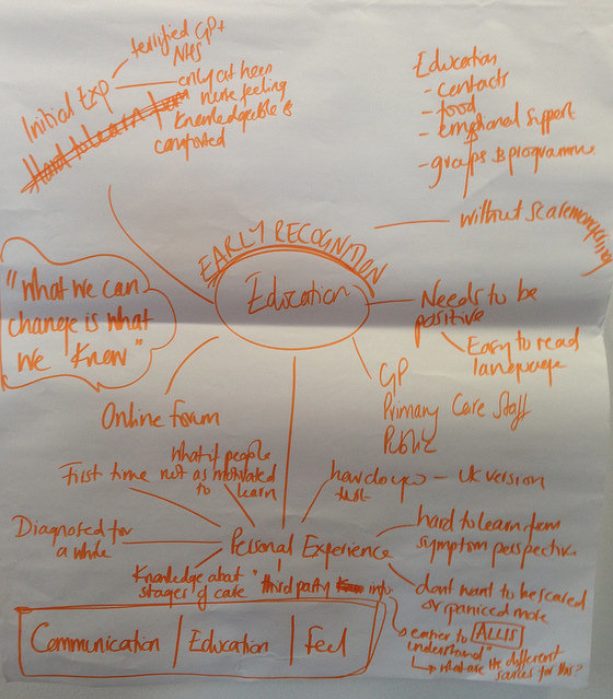
Group discussion summarised
In summary, three key themes emerged from this conversation:
- Supporting people to ‘get the information they need ‘ from their GP
- Supporting people to approach third sector organisations (like Chest Heart and Stroke and the British Heart Foundation) for advice and support and to get tips and support from practitioners and peers
- Supporting public awareness raising to support earlier diagnosis
This led the group to identify what was needed, namely…….
How do we support or challenge GPs – and maybe practice nurses too?
- Through complaints?
- Forum with GPs
- Small scale pilot – sharing success of this with others
- Training and educating GPs eg the British Heart Foundation said that they could offer training to front of house staff and GPs
- Tools to improve patients’ conversations with GPs eg list of questions to ask at appointment/pre-consultation resources to help empower people and/or prepare them before they go in to see the doctor
- We heard that in England GPs are being inspected – covering clinical practice to health promotion over next 3 years. A framework has been established, with a scoring matrix used. They contact a cross-section of patients by telephone and may for example, select patients from the heart failure register and ask them how happy they are with their treatment.
- There was some preference from within the group for making greater use of nurses in GP surgeries; seen as an under-used resource who can provide support but also identify when you need to see the GP. They should be targeted too in any initiative/education drive/ training offer or ‘bundle’.
- Chest, Heart and Stroke’s Voices programme is designed to train and empower people.
- Could we go to GPs with an offer of help?
- Should we also be thinking about ‘What I want the GP to ask me?’
The group discussed that this is in the context of:
- Increased focus on self-management and noted how this all interacts with the different parts of the system
- More referrals from GPs to Social Work – signposting to them and to 3rd sector/party organisations.
- More people are being re-referred to GPs. Support groups in Scotland are patchy and focused on people at end of cardiac rehab
- Exercise is often offered but not something everyone is interested in. CHS are growing more social groups, including online eg Facebook.
- More generic groups can offer support eg focused on long term conditions and not just heart failure, people may prefer to get involved in groups focused on their interests.
- Social Media
- Some groups are closed. Issue as to whether this identifies people with heart failure or not as online links can be traceable – some people don’t mind; others don’t want their neighbour to know they have heart failure.
- Some patient forums, including the British Heart Foundation’s, aren’t moderated. This means that people can post up ‘wrong’ information that goes unchallenged and can lead to spread of mis-information. Moderator needed?
- Issue of online trolls
- Things not being joined up
- Is there a disconnect between GPs and cardiologists? If a patient is diagnosed with an acute condition by a cardiologist, it becomes more difficult to access the GP as the patient is ‘no longer under primary care.’
- The heart failure nurse isn’t copied into all correspondence, so may not have all the necessary information about a patient’s care or condition.
- There can be a lack of certainty over where to go for advice or for practical support.
Revisiting community mapping
This part of the day was to explore the content and functionality of local information that was already available. As we’d already covered some of this ground during ‘homework feedback’ we focused our time on looking at some of the following sites – as possible inspiration for the work North Lanarkshire Council has undertaken to do around improving local online information for people with heart failure.
- East Dunbartonshire Assets map
- Google maps – free, slightly less sophisticated than above – lots of examples out there!
- Voluntary Action North Lanarkshire ( see Locator)
- Voluntary Action South Lanarkshire ( see Infobase and Locator search)
- ALISS
- Living it Up (Flourish) and its No Delays prototype which can be found from this page
- There’s also the Living it Up experience guide to ‘Living with heart failure’
Developing plans for what we want to pilot/trial
We started out from the basis that by the end of today we wanted to agree ideas that we wanted to test. Ideally, a minimum of two and maximum of four, with responsibility for delivering them shared across the group.
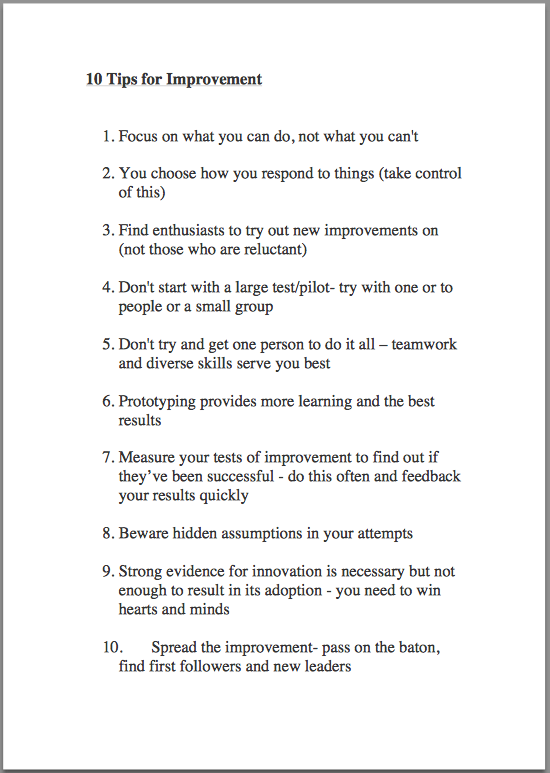
The group were reminded:
- To focus on what we can do (and not what we can’t)
- We have three months until the end of December to do this within the timeframe of the project
- No budget to support these ideas apart from our time, energy, commitment and expertise (unless project partners can provide or secure funding)
- Top 10 tips for Improvement
We also took some time to consider what we’d hope to achieve and our earlier potential improvement ideas. Interestingly, the discussions we had had earlier that morning had really shifted on the group’s thinking – very much away from peer support groups for example, to focusing attention on achieving earlier diagnosis and raising awareness.
Next step – agreeing ideas to test and setting up working groups
These are the ideas the group came up with instead.
We then asked the group to vote on their favourite. They were given four red dots each which they could allocate however the liked – so they could spread these among the three ideas or give them all to one.

Voting on favourite improvement ideas
The top three ideas were around:
- patient information – developing a pre-diagnosis symptoms pathway
- engagement with GPs/nurses/pharmacists
- raising public awareness
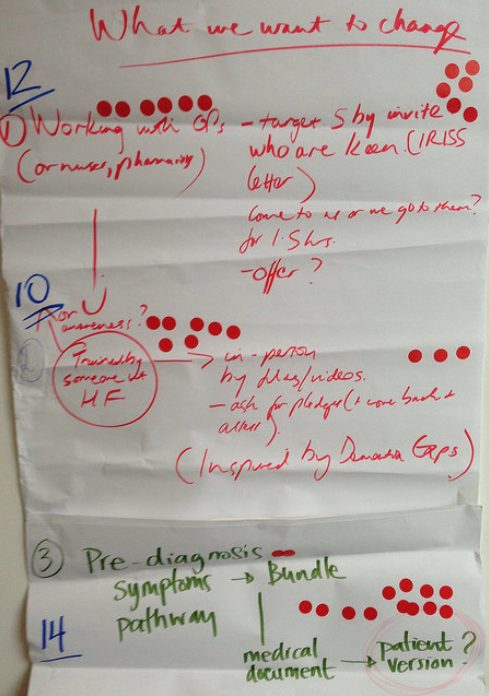
Top scoring improvement ideas
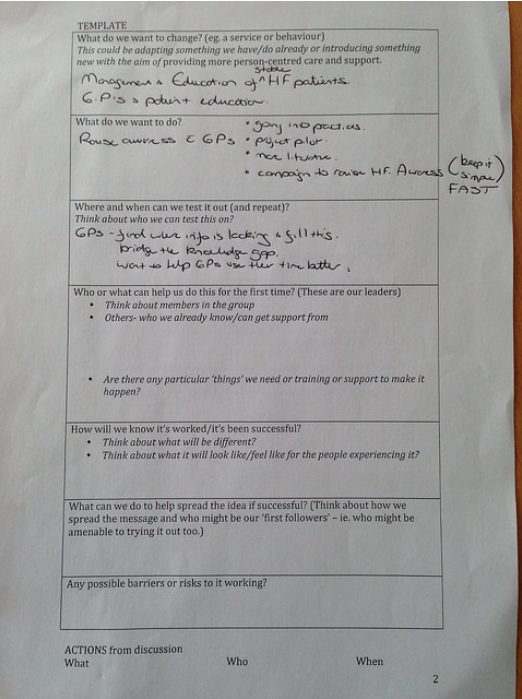
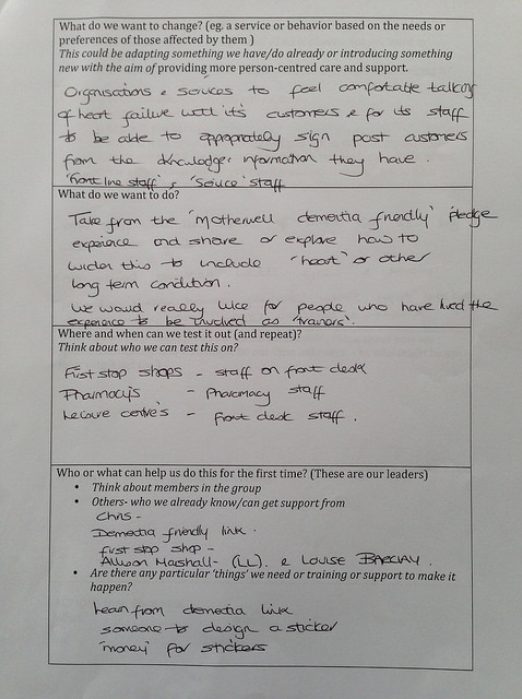
At this stage we split the group up into three smaller groups to create a plan for each of the ideas. We supported this by giving people a template to work through. Each group then fed back to the whole group about their plans and invited comments, feedback, and asked for any help others may be able to provide. Here the three completed templates:
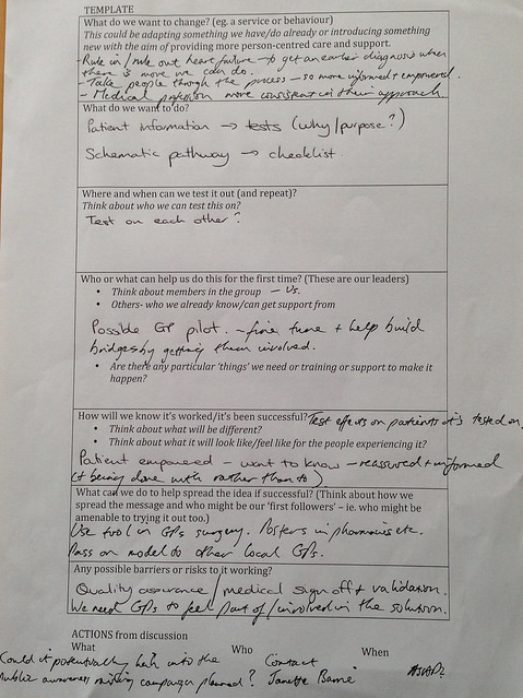
The fourth idea (which we don’t have a photographed template for) is the improvement of North Lanarkshire Council’s online resources, working with individuals in the group to improve local information.
Last, but not least, we invited people to allocate themselves to a working group to make these plans a reality. People were encouraged to be on more than one working group if they wished.
Homework and plan for next meeting
For homework, we encouraged each group to be in touch with each other before the next session to take these plans forward. We felt the next meeting should include:
- Reports from each working group on progress
- Focus on how to measure impact and learn from any tests of improvement
- Discussions about how to share/spread improvement ideas to others
- Discussions about what would happen at the end of this project
Feedback and evaluation
All smiley faces (10 out of 10). Sorry I didn’t get everyone into the picture

What went well?
- The soup was lovely!
- Feedback on the homework from the last session was really valuable
- Good to have British Heart Foundation there too!
- Good balance in group between professionals and non-professionals
- No TLAs (third letter abbreviations)
- We’ve moved forward.
- Interaction and talking
What didn’t work so well?
- Confusing tea bags!
- A bit cold in the room
- Wi-fi in building!
- The facilitators found going off the agenda, esp with regard to timings stressful, but group members welcomed this and the flexibility
- Less parking than first venue (but no stairs which is good)
What will you take away from the day?
- Feeling rejuvenated!
- We have actions plans!