Review, re-cap, repetition and reinforcement
Still in the learning stage of our work we used the start of this meeting to re-state project aims, re-cap what we understood by co-production and person-centred care and re-visit our working together agreement.
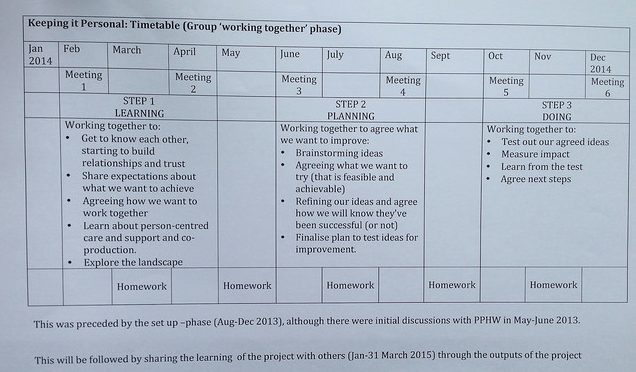
We also discussed our hopes and ambitions for this work in the context of the project timetable so people could see how these hopes and aspirations may fit into this trajectory. Despite stressing the need to allow for time to build up relationships, learn together and establish solid agreement, this group’s desire to move quickly to action was quite tangible. Showing them where we were as part of a project plan was, I hope, quite helpful in keeping everyone on board.
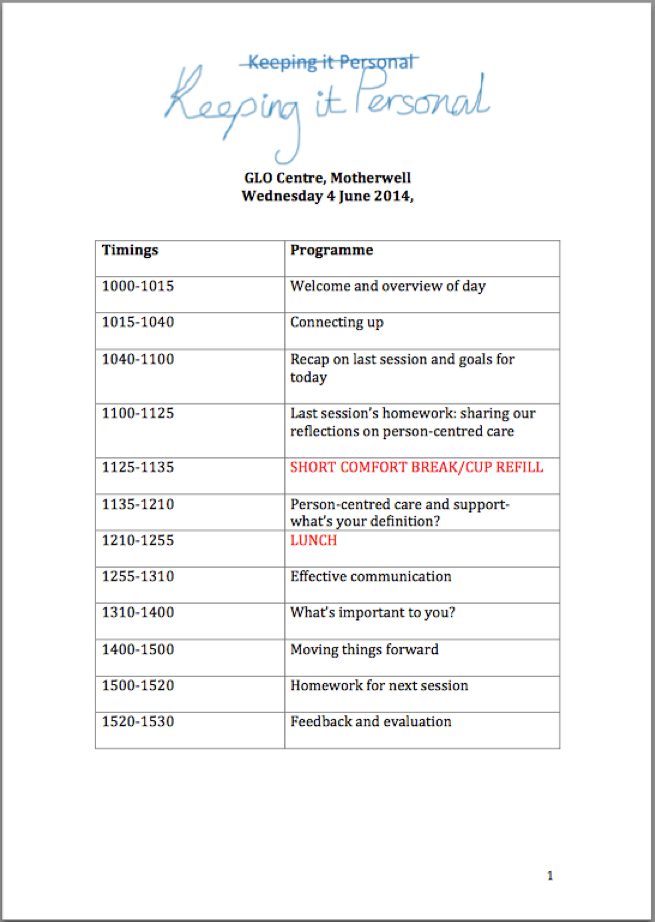
This was our programme for the day and our goals were:
{kind=link}
- To understand person-centred care
- To understand the assets we have, how we can optimise them and help each other
- Agree our homework and decide ‘what’s next?’
Connecting up: the power of positive thinking
As our ice-breaker we asked people to speak in pairs about what keeps them strong (before moving to repeat with a new partner).
A summary of thing people shared include:
- Having goals or being determined
- A positive mental attitude
- Glass half full rather than half empty attitude
- Time to oneself/’me time’
- Music
- Doing things one enjoys eg a bit of pampering or the football or gardening
- Being loved by family/encouraged by others
- Being needed by others
- Pets
- Being pampered
- Holidays
- Speaking to others in a similar situation to myself
Defining person-centred care
There is no clearly defined or agreed definition of person-centred care. As the 2014 Health Foundation publication ‘Helping measure person-centred care’ explains, the lack of a definition means there can be challenges evaluating this approach. However, I like Andy Crawford’s view (Head of Clinical Governance at NHS Greater Glasgow and Clyde), that “whatever ‘it’ is, ‘it’s’ negotiated”.
We shared other perspectives on what person-centred care means to help start this discussion and showed the group:
A GP’s perspective
[youtube]https://www.youtube.com/watch?v=y43TLRzal44[/youtube]
The view of a person who is self-managing their own care
[youtube]https://www.youtube.com/watch?v=x7Zu4P1qK48[/youtube]
Group members then shared their homework which covered:
- Reflections on what person-centred care and support meant to them
- What people thought person-centred care and support should look like
Group members reflections included that :
- services need to be better co-ordinated around the individual
- people should be offered choice rather than told what services will be put in place
- there needs to be more recognition of the role of professionals other than GPs and consultants in providing advice and support
- people need to be given enough time to discuss their support needs
After this discussion we felt that it would be useful for the group to create their own language and vision of person-centred care. This might help people feel confident talking about it and challenging other people’s views. So we asked people to form three small groups and devise a person-centred campaign.
Person-centred campaign
We asked each group to consider what their campaign message should be, how should it should be presented and where it should be communicated. We provided groups with examples for inspiration. These included: NHS Scotland’s ‘5 Must Do with Me’ areas ‘ and the Principles of Person-centred care and support developed for the Person-Centred Health and Care Collaborative to ‘help find the words and change conversations.’
Each group chose to design a poster
Group 1 aimed to promote the benefits of real partnership working, their strap line was: ‘Getting further together – we all have our part to play’
Group 2 focused on empowering individuals and promoting choice, they chose the strap line: ‘Who cares? …I do’
Group 3 used the strap line ‘Take CARE’ with the letters CARE representing: Control (individuals taking control), Acting on symptoms, Responsibility (for self), Expert (using own as well as professional expertise)
Here are short videos of each group describing their campaign
Effective communication
“The biggest problem with communication is the illusion that it has taken place.” (George Bernard Shaw)
The notion that ineffective communication is a hidden problem was introduced – people hide misunderstanding. We know that much of what patients are told by their doctors is forgotten or misunderstood. This is well-illustrated by this clip from the American TV programme, ‘House’ about a clever but awkward and flawed MD.
As miscommunication is so well documented and a common difficulty people experience, we decided to introduce ‘Teachback’ to the group. Teachback involves professionals checking people’s understanding by asking them to repeat back what has been said. At the same time working to improve their skills in being able to explain things in simple language, by not using jargon or medical terms. Health literacy after all is about the ability to access, understand and action information.
We used a Scottish Government DVD resource to introduce Teachback. There were no examples that were specific to heart failure, so we chose one about a woman being recommended to have an HIV test.
Interestingly some group members had negative reactions to the DVD. They did not think Teachback would be an effective approach to improving communication at a time of crisis, for example at a point of diagnosis, or when raising a serious issue for the first time. Instead people felt this approach could be more effective when working with someone to manage a condition over time. For example, when attending for check ups.
Perhaps this American example which aligns to the group’s feedback fits this description and would have been better? We’d avoided using this earlier as comments from the other group indicated examples from other countries could be confusing due to the different context.
What’s important to you (WITTY)?
WITTY was developed as part of IRISS’ project called ‘Social Assets in Action‘. From this project a free version of WITTY was made available for use on an i-pad, but a paper version can also be used.
WITTY is designed to help people create a personalised visual map of what’s important in their life to promote well-being. In our group we asked people to work in pairs and use a paper tool (concentric circles), placing themselves in the centre of the circle and what was important to them closer or further away from them based on their own perspectives. Things people may place in the circles could include: pets, social groups, places, activities and experiences that are important to them. People can be given the option of writing on the paper circles or using props – like lego pieces to represent what is important to them.
The exercise
In pairs, people asked to take turns using the WITTY resource. We asked one person to complete WITTY and talk through what they are doing and what the aspects on the map mean to them, and we asked another person to listen and summarise what the other person said at the end of the exercise. We reminded people that it’s ok to stop people to check for clarification about what they have just said, and also to observe and take notes. We also asked people to bear in mind and possibly apply the Teachback technique.
A personal example of what was important was offered by someone in our group. This included:
- The most important people to me are my wife and my family and their wellbeing
- Cooking is important to me and
- Gardening and cycling
- Doing volunteer driving
- I’m close to my brother, sister, mother and aunt.
- Housework’s important, but it’s on the outer ring!
- What I’d like more of: holidays and meals out with friends
Following the exercise we asked for group feedback on how they found the exercise using the following questions.
A) What’s the difference between asking: What’s the matter with you? and, What matters to you? People responded by saying:
- It’s broader
- Less negative/more positive
- WITTY helped reveal relationships between different things/people to help you cope
- The general view was that it was ‘quite easy’ to have a conversation around ‘What’s important to you?’
B) How easy/difficult was it to communicate with each other during the exercise? People responded by saying:
- The general view was that it was ‘quite easy’ to have a conversation around ‘What’s important to you?’
- Good with someone I don’t know
- Good at prioritising and sharing
C) How and when do you think you could you use these tools and techniques? People responded by saying:
- Mapping life – shows the positives and good things
- Can also show bits in life that are lacking (and help you plan)
- Might identify lots of ‘paid’ support but not ‘natural’ ones – can then help build those up and make connections.
- Helps you open up and can help establish relationships
- May depend on who is using it – barriers may naturally go up with some (eg a GP?)
- Helps you be more comfortable with new services
- Need to be genuine – the person using the tool needs to be really interested
- Helped show the relevance of Teachback (when maybe not seen before)
There was also discussion around the fact that some people used these techniques naturally, however, this was not true for all and the value of having tools to support this was agreed.
Moving things forward and homework for next time
We took the opportunity to revisit the 16 ideas-North Lanarkshire identified at the previous meeting as potential actions (or future improvement activities) and asked the group:
- Have any of these already been done?
- Should any be actioned for next or next again meetings?
- Should any be parked for now (with scope to bring back later if we want)
- Are future improvement activities something we want to consider implementing at a later stage in the project?
We split group into three smaller groups and asked people to plot the ideas in three areas: things people still needed to learn about, things they were planning, or were already doing.
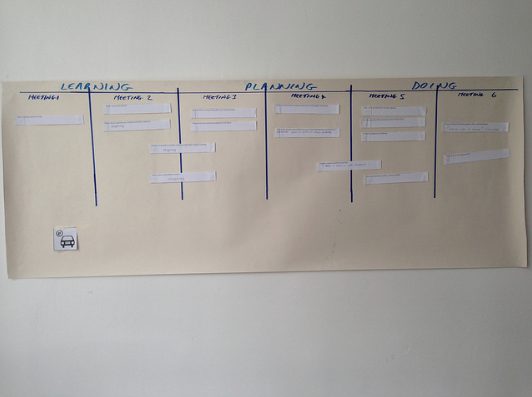
Capturing learning, planning and doing activities
This approach was useful as it helped us identify similarities and differences of opinion about the ideas amongst the whole group. Consequently we discussed the ideas and identified the kind of things we needed further clarification about. This list of potential ideas for improvement was created as a result of this discussion.
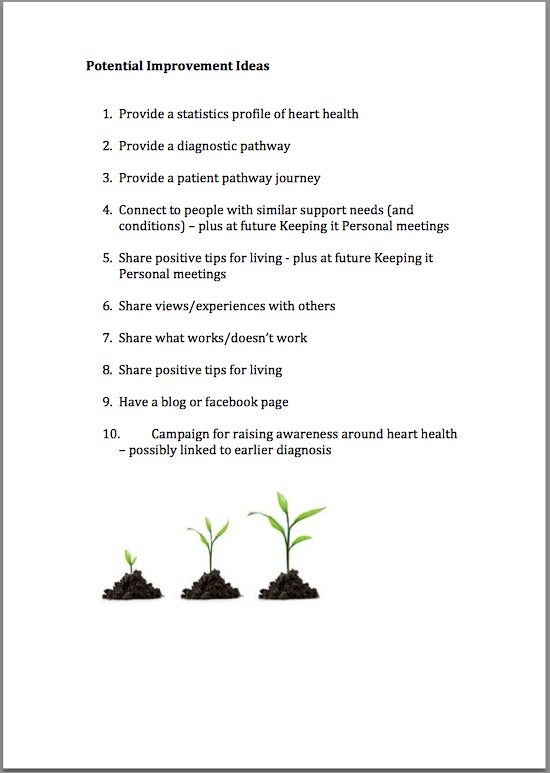
We also created a plan to ‘move things forward’.
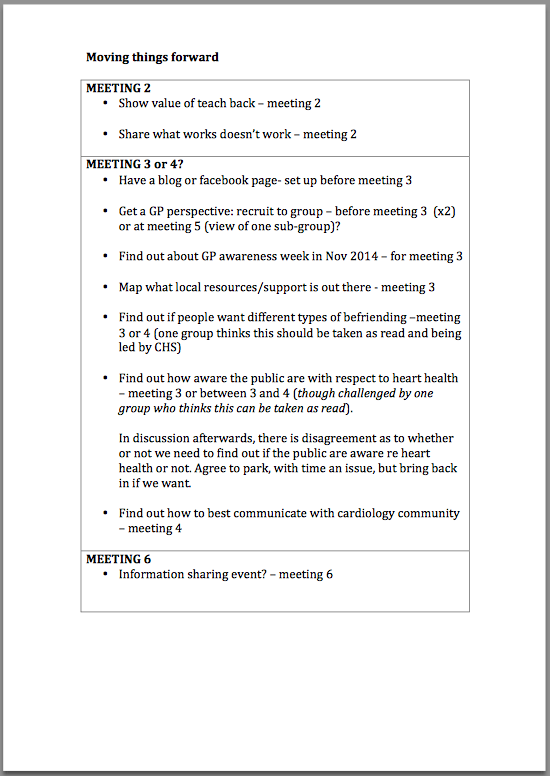
Feedback and evaluation
As with all meetings, at the end we asked for general feedback, a gut reaction response. People were given smiley, not so sure and unhappy faces to hold up to share their gut reaction to the session. The response included smiley faces and two not so sures.
What went well?
- Taking stock and direction
- Good to see everyone again
- Learnt about new things eg teachback
- All mixed well
- What keeps me strong exercise and ideas.
What could have been better?
- The photos! (taken for the personal profiles)
- Be good to have a bell!
- Timings – felt that we tried to cover too much in the time for some; a 5 min warning before the end of sessions and people taking personal responsibility for listening to this (see above!)
What will you take away from today?
- Clearer about progress and what meetings are about
- Continued sense of sharing and learning together